MFEL3010: Medicine for Students of Natural Sciences and Technology
Tips: Practice on exam questions through Kognita
Cells, Tissues and Organs
Four basic tissue types:
- Epithelial tissue: lines surfaces in the body.
- Muscle tissue: is made up of fibers that contract.
- Nervous tissue: consists of cells with projections that transmit electrical signals for communication.
- Connective tissue:
- Loose connective tissue: acts as padding under skin and elsewhere. In a soft extracellular matrix.
- Bone: made up of cells in a hard or stiff extracellular matrix.
- Cartilage: made up of cells in a hard or stiff extracellular matrix.
- Blood: made up of cells in a liquid matrix.
Differentiation of cells: Different cells express different genes (making different proteins).
- Ectoderm: gives rise to skin and nervous system.
- Mesoderm: give rise to muscle, skeleton and organs of circulation, reproduction, and excretion.
- Endoderm: give rise to lining of gut and associated organs.
Basic cell structure:

- Nucleus
- Cytoplasm containing organelles
- Cell membrane: double lipid layer where each molecule has one water soluble and one lipid soluble end.
Cell function:
- Inheritance (DNA)
- Cell metabolism (utilization of energy, Adenosine triphosphate)
- Protection and support (production and secretion of proteins)
- Motion (due to specialised proteins within)
- Communication (transmit and receive electrical and chemical signals)
DNA:

- DNA curls around proteins to form chromatin and then chromosome.
- DNA replication.
Mitosis:
Mitosis is a part of the cell cycle when replicated chromosomes are separated into two new nuclei.

- Late interphase (
$G_2$ ): cell check for complete DNA replication. - Prophase: chromosomes condense, become visible. Spindle apparatus forms.
- Prometaphase: Nuclear envelope fragments. Spindle fibers attach to kinetochores.
- Metaphase: Chromosomes align along equator of the cell.
- Anaphase: sister chromatids separate to opposite poles of the cell.
- Telophase: nuclear membranes assemble around two daugther nuclei. Chromosomes decondense. Spindle disappears.
- Cytokinesis: Division of the cytoplasm into two cells.
- Early interphase (
$G_1$ ): cells resume normal functions or enter another division cycle.
The interphase is divided into three phases:

Meiosis:
- reduction division (half of the chromosomes in each) and
- equational division (split chromosome)
Amino acids:
(building blocks of proteins) 21 amino acids, each is coded by a triplet of bases in DNA and RNA.
Protein synthesis:

- Replication: DNA duplicates
- Transcription: RNA synthesis (DNA used to form RNA)
- Translation: protein synthesis at the ribosomes
This process is unidirectional - genetic information can only flow one way.
Protein structure:

- Primary: amino acid sequence (polypeptide strand)
- Secondary:
$\alpha$ helix or$\beta$ pleated sheet - Tertiary: 3D structure of monomeric and multimeric protein molecules
- Quaternary: coupling of more molecules to a larger molecule.
Some terminology:
-
Ribosomes: site of protein synthesis. Composed of a large and a small subunit. Can be free or attached to the endoplasmatic reticulum.
-
Organelles: Small specialised structures with particular functions.
-
Cytoplasmic skeleton: Supports the cell and moves in accordance to the cilia and changes in cell shape. Consists of microtubules (hollowness, tubulin [protein]), microfilaments (structure, actin [protein]), and intermediate filaments (mechanical strength).
-
Endoplasmatic reticulum (ER)
- Rough ER: Produces and modifies proteins. Has ribosomes attached.
- Smooth ER: Manufactures lipids. No ribosomes attached.
-
Golgi apparatus: modification, packaging, distribution of proteins and lipids for secretion or internal use. Flattened membrane sacks stacked on each other.
-
Mitochondria: major site of ATP synthesis, increase in number when cell energy requirements increase. This is aerobic metabolism. The anaerobic metabolism take place in the cytosol, but result in very little ATP.
-
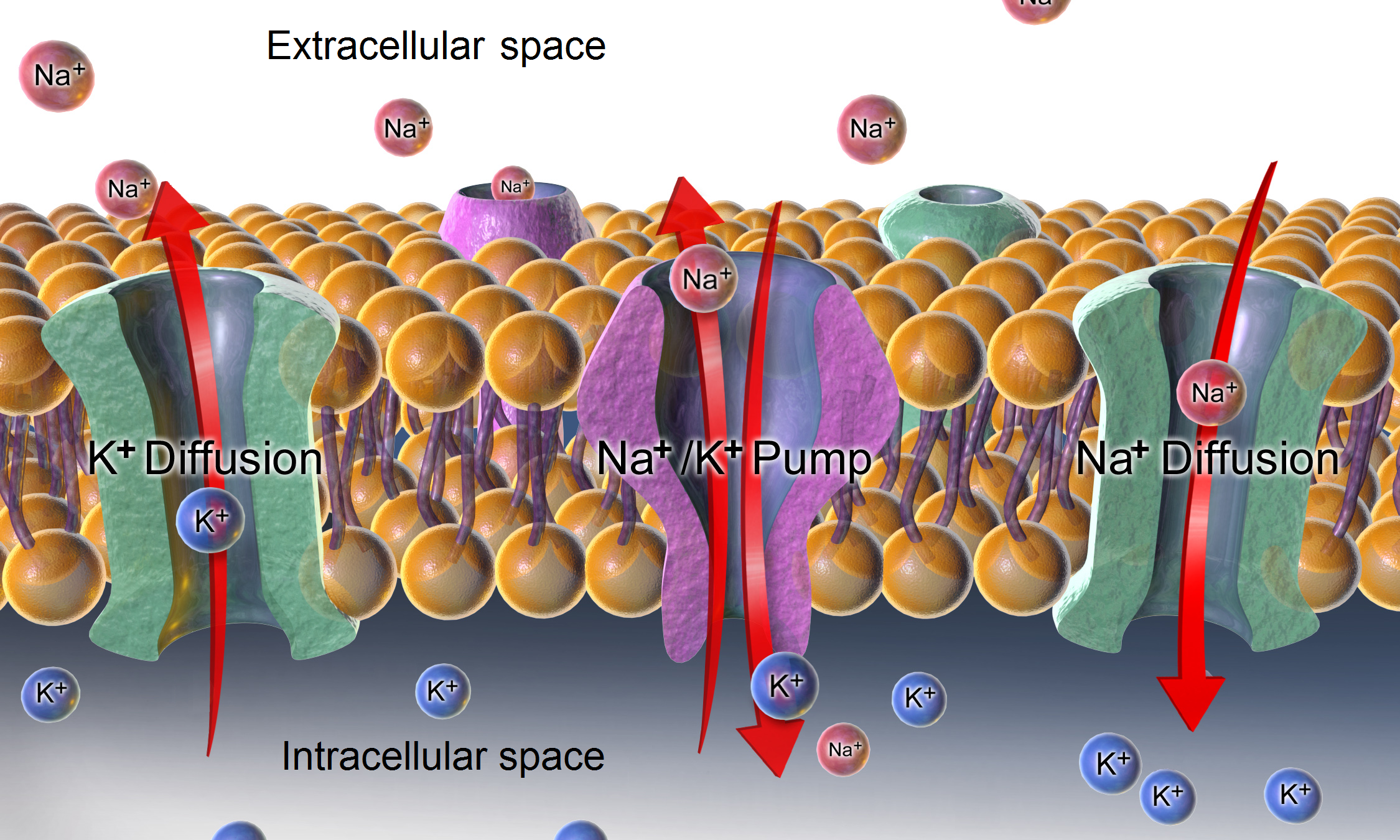
Membrane proteins: Important parts of the cell surface membrane, markers, attachment sites, channels (move through by diffusion, osmosis, filtration), receptors, enzymes or carriers. Responsible for the binding of peptide hormones.
-
Passive transport:
- Diffusion: concentration gradient driven.
- Osmosis: diffusion of solvent across selectively permeable membrane due to concentration gradient in solute. Hypertonic: cell shrink; isotonic: cell remains the same; hypotonic: cell swells.
- Filtration: pressure gradient driven.
-
Active transport: Transport against a concentration gradient. Requires energy (ATP).
-
Endocytosis: Internalisation of substances by formation of vesicle.
-
Exocytosis: Accumulated vesicle secretions expelled from cell.
The sodium potassium pump:
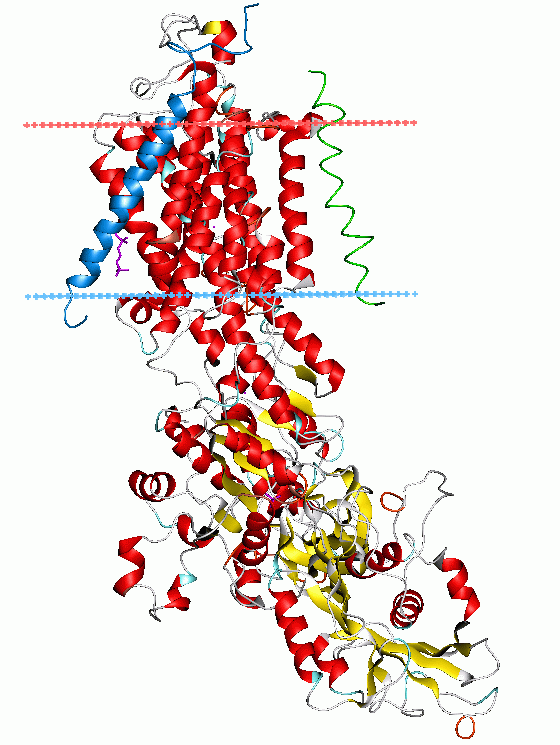
This process is responsible for maintaining the large excess of
Depolarisation: Inside of cell becomes less negative. Caused by inflow of
Repolarisation: Inside of cell becomes more negative (from depolarisation to resting potential). Caused by diffusion of
Action potential: A cell can depolarise itself by generation of action potential. Once the membrane potential reaches the treshold potential, the depolarisation becomes self perpetuating. The channels open and cause an inward flow of
Signal conduction: Action potential in one part of the cell membrane causes threshold depolarisation in neighbouring part, triggers local action potential which travels along cell.
Cancer

Cancer is a group of diseases where control over cellular proliferation has been lost. Depending on the type of cancer, the cells have varying tendency to invade the body. Spread through blood stream and liver from the intestines and through the lymphatic system.
- Unhibited cellular proliferation: Control over the cell population is lost.
- Invasion of surrounding tissue: The cells penetrate cellular and tissue barriers.
- Angiogenesis: The cells ''attract'' blood vessels to supply themselves.
- Metastasis: The cells are able to settle and proliferate elsewhere.
Disease of mutations
- ~5-7 mutations in relevant sites of the DNA to change a normal cell to a cancer cell. Mutated cells accumulate as the years go by → more common in elderly.
- Mutations in these classes of genes may cause cancer: (proto)oncogenes (mutated growth regulatory genes), tumor supressor genes (regulating cellular growth and death) and mutator genes (genes repairing DNA / removing mutations).
- What causes mutations? Ionising radiation, chemicals, virus and spontaneous injuries (replication error, endogeneous metabolites).
- Familial cancer (HNPCC): born with one defect in one of the two DNA enzyme repair (in every cell).
Treatment
- Surgery: when the tumor is technically and biologically operable. Often palliative (symptomatic) surgical treatment.
- Chemotherapy
- Radiation: attack the cell cycle at different stages.
- Specific (''biological'') treatment
DNA Analysis
What is DNA?

- Our genetic material, called DNA (deoxyribonucleic acid), can be seen as an instruction book for how we are made.
- Our DNA is made up of ~20.000 genes.
- DNA contains 4 different bases (A, C, G and T).
- DNA consists of ~3 billion bases.
- The order of the bases determine how we are made.
- The order varies between individuals. This is called genetic variation. But more than 99.9 % of the DNA are the same in all people, so less than 0.1 % of the DNA is responsible for the differences from person to person (length, hair color, risk of diseases, etc.).
- The bases pair up with each other, A with T and C with G, to form units called base pair.
- The base pairs are arranged in two long strands that form a spiral called a double helix.
- The DNA is organized in 23 pairs of chromosomes. Every person inherits one set of 23 chromosomes from the mother and one set of 23 chromosomes from the father.
Where do we find DNA?
- Blood, semen, saliva, mucous, tears, urine, feces, vomit, bones, teeth, skin cells, hair. IN EVERY CELL!!!
- Most of the DNA is located in the cell nucleus (nuclear DNA), but a small amount of DNA (37 genes) can also be found in the mitochondria (mitochondrial DNA).
How do we isolate DNA?
To be able to analyze DNA we have to extract the DNA from cells in a relatively purified form. Basic steps:
- Chose your source of DNA (for instance blood).
- Break the cell membranes to get all the cell contents in solution.
- Remove proteins and other cell components that you are not interested in.
- Precipitate the DNA by adding salts and ethanol.
- Re-solve your DNA dilution in some solution (water/buffer).
How do we analyse DNA?
- Sometimes we have only a very small amount of DNA available for analysis (for instance DNA samples obtained from crime scenes). To increase the amount of DNA, these samples are subjected to the Polymerase Chain Reaction (PCR), which is a technique that copies DNA by amplifing small amounts of DNA into several thousand copies.
- To be able to study DNA, we often begin by cutting the DNA strand with restriction enzymes. Restriction enzymes works like a pair of scissors, that cuts the DNA strand at particular sites. This particular method of comparing DNAs is known as restriction fragment length polymorphism (RFLP). IMPORTANT! The fragments will have different length from individual to individual based on the small differences in DNA that exists between humans.
- Gel electrophoresis:
- DNA samples already cut with restriction enzymes are added to a gel and subjected to an electrical field.
- DNA fragments has a negative charge and moves slowly towards the positive end.
- Shorter fragments travel through the gel faster than longer fragments.
- DNA is visualized using fluorescent dyes.
- DNA microarrays: DNA microarrays is a collection of microscopic DNA spots attached to a solid surface. DNA microarrays allow us to study >1 million locations on the DNA strand in one single sample. Often used to study something called Single Nucleotide Polymorphism (SNP). A SNP is a difference in one single base at a particular place on the DNA strand. Differences in SNPs are sometimes the cause of disease.
- DNA sequencing: DNA sequencing is the process of determining the precise order of nucleotides within a DNA molecule. DNA sequencing may be used to determine the sequence of individual genes, larger genetic regions, full chromosomes or entire genomes.
Why do we analyse DNA?
- Forensic DNA analysis (to tie a person to a crime). Using gel electrophoresis in forensics are known as DNA fingerprinting.
- Paternity testing (to test whether people are related).
- In research:
- Purpose: Determine inherited factors that predispose to disease, and compare DNA samples from a large group of sick subjects with DNA samples from a large group of healthy subjects to find parts of the DNA that differ between sick and healthy subjects.
- Aim: To learn more about the disease and find potential targets for gene replacement therapy and/or gene testing.
- Common used method: Analyzing a large number of single nucleotide polymorphisms (SNPs) using DNA microarrays or DNA sequencing.
- In the clinic:
- Newborn screening: Identify genetic disorders that can be treated early in life.
- Diagnostic testing: To diagnose or rule out a specific genetic disease suspected based on symptoms.
- Carrier testing: To identify people who carry one copy of a gene mutation that, when present in two copies, causes a genetic disorder. Relevant for individuals who have a family history of a genetic disorder to determine the risk of having a child with a genetic condition like cystic fibrosis.
- Prenatal diagnosis: Detect changes in a fetus's genes or chromosomes before birth. This type of testing is offered to couples with an increased risk of having a baby with a genetic disorder.
- Predictive testing: Estimate the chances of developing disorders with a genetic basis, such as certain types of cancer. For example, an individual with a mutation in the gene BRCA1 has a 65% lifetime risk of breast cancer
- Pharmacogenomics: To determine the appropriate dosage of some medications. For instance, there are large inter-individual differences in dose need of the blood thinning drug Warfarin. This is largely determined by two variations in DNA. If these variants are determined, a more appropriate dose can be prescribed, avoiding serious side effects of the drug.
The Nervous System

Organisation
- Central nervous system (brain and spinal cord) integrative and control centers.
- Peripheral nervous system (spinal nerves with branches, and nervous mesh in internal organs) communication lines between the CNS and the rest of the body.
- Sensory (afferent) division (somatic and visceral sensory nerve fibers) conducts impulses to the CNS from receptors.
- Motor (efferent) division (motor nerve fibers) conducts impulses from CNS to effectors.
- Automatic nervous system (visceral motor, involuntary) conducts impulses from CNS to cardiac muscles, smooth muscles and glands.
- Sympathetic division: mobilises body systems during activity, i.e. increase blood pressure, reduces blood flow to internal organs and increase heart rate (''fight or flight'').
- Parasympathetic division: conserves energy, promotes ''housekeeping'' functions during rest, i.e. increase visceral activity, reduce blood pressure, increase blood flow to internal organs, reduse heart rate.
- Somatic nervous system (somatic motor, voluntary) conducts impulses from CNS to skeletal muscles.
- Automatic nervous system (visceral motor, involuntary) conducts impulses from CNS to cardiac muscles, smooth muscles and glands.
Functional unit - the neuron
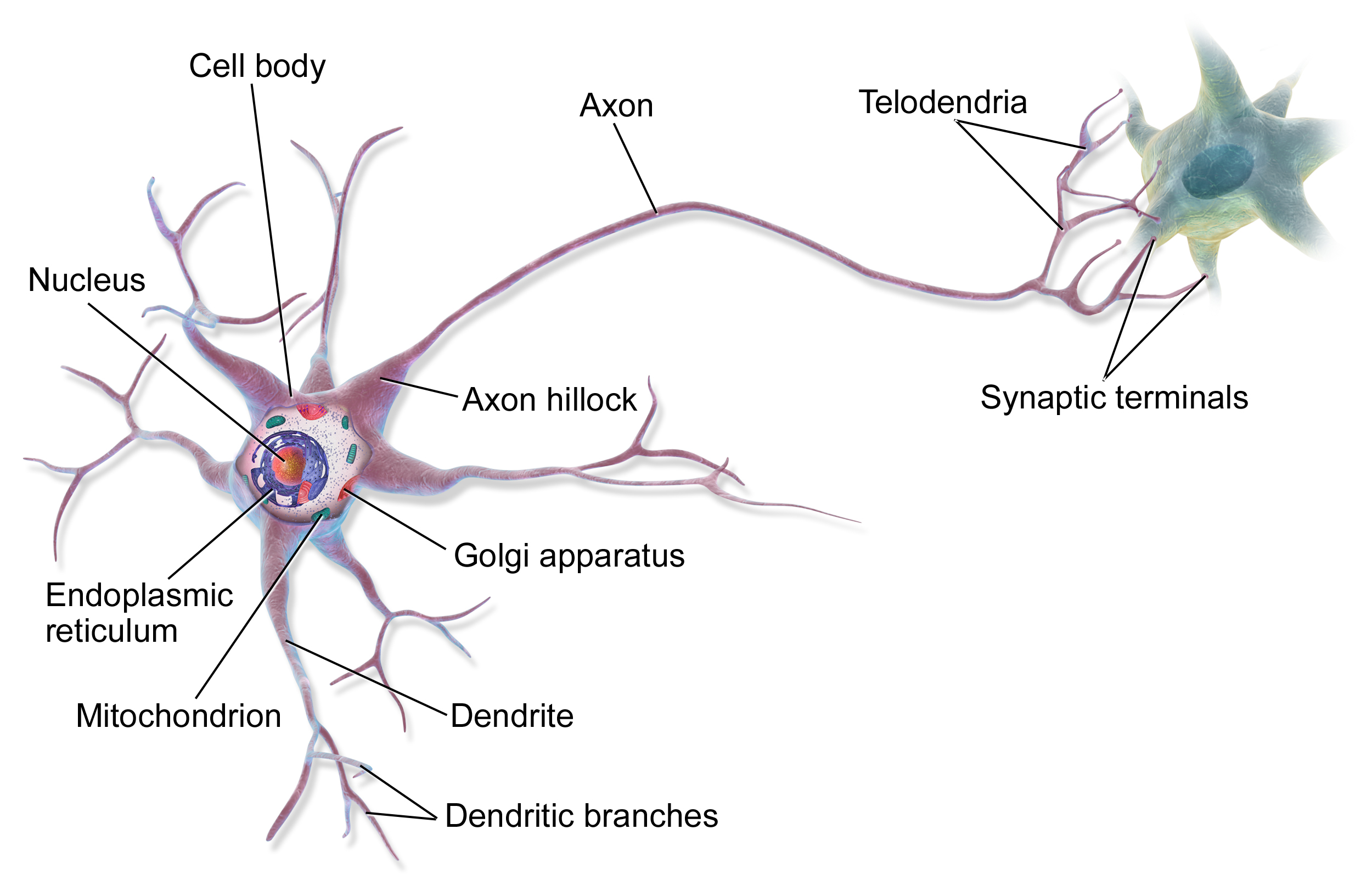
- Each nerve cell consists of a cell body and various branches. The main brach is called the axon. The axon terminals transmit signals while the dedrites receives signals.
- Conduction: Dendrites receives electrical signals, the cell body integrates incoming signals and generates outgoing signals to the axon which passes the electrical signals to dendrites of another cell or to an effector cell.
- Signal transmission: Synapses are transitions between nerve cells and another cell (e.g muscle cells, glandular cells, or even other nerve cells). Action potential in presynaptic cell triggers
$\text{Ca}^{++}$ influx which again triggers release of vesicles with signal substance - transmitter diffuses across gap. Binding of transmitter in postsynaptic cell opens$\text{Na}^+$ channels: triggers (or inhibits) action potential, excitatory or inhibatory. The total input from other nerve cells generate a chemical environment that controls the output of a nerve cell. - External drugs can: mimic the action of transmitters, increase the level of transmitters, or block the action of transmitters.
- Glia cells: myelin coiled around axons form isolating fatty sheets which increase conduction speed. Myelin sheets main function around the nerve fiber is increasing conduction velocity
The central nervous system
- Grey matter: mostly cell bodies.
- White matter: mostly axons with myelin sheets (fat).
- Cerebrospinal fluid: protect brain when in movement.
- Multiple sclerosis: loss of myelin (slower conduction).
- Brain: Cerebrum with cortex (conscious experience and voluntary activity) and thalamus (sensory input routing), cerebellum (coordination), brainstem that includes pons (maintains consciousness) and medulla oblongata (autonomic control, that is it regulates heart rate, respiration, blood pressure, etc. and acts unconsciously).
- Frontal area have the main governing of rational behaviour.
- The limbic system: emotions and activities related to regulation of temperature, osmolarity, appetite, smell, sex.
- Hippocampus: process impressions to long term memory
- Memory: 1) Short term memory; and 2) Long term memory can be declarative (semantic: stored as terms/words; episodic: stored as smells, senssations, etc.), or procedural memory (skills).
- Pain: 1) Acute pain; 2) Referred pain, pain from inner organs may feel like originate from skin; 3) phantom pain, apparent pain in amputated limb.
The Heart and Circulation
The circulatory system: heart, blood vessels and blood.
Blood:
- Plasma: water, electrolytes and proteins
- Cells: white blood cells (leukocytes), blood platelets (thrombocytes) and red blood cells (eryhtrocytes)
Transport:
- oxygen from the lungs
- carbon dioxide to the lungs
- nutrients from the intestine
- waste products to liver and kidneys
- signal substances (hormones) to the entire body
- electrolytes and proteins to equalise the internal environment
- white blood cells and antobodies for immune defence.
Heart muscle
Conducts and contracts! The action potential triggers the intracellular release of
Relaxation: elasticity of the cell returns it to original shape.
-
The Heart cycle:
-
Right atrium: receive oxygen depleted blood from the body
-
Right ventricle: pump oxygen depleted blood to the lungs
-
Left atrium: receive oxygen rich blood from the lungs
-
Left ventricle: pump oxygen rich blood out of the heart to the body. Flow in at low pressure and out at high pressures.
- Diastole: muscle relaxation, pressure drops, and blood flows into the ventricles from atria and veins.
- Systole: muscle contraction, pressure rises, and blood is ejected from ventricles intro arteries.
-
-
Myofibrils: a basic rod-like unit of a muscle cell
- Myofilaments: the filaments of myofibrils, constructed from proteins, principally myosin or actin. Various arrangements of myofilaments create different muscles.
Useful formulae
Stroke volume (SV): The difference between the End Diastolic Volume (
Cardiac output (CO): Product of Stroke Volume (
Ejection fraction (EF): A measure of ventricular muscle power (%),
Blood vessels

Large vessels saves up elastic energy from the increasing pressure in systole; then uses this energy to squeeze / pump blood in diastole. Medium-sized vessels gives resistance to flow and regulate central blood pressure. Local resistance direct blodd flow to organs where it is most needed.
- Total peripheral resistance: Product of resistance (
$R$ ) and flow ($Q$ ):$$P = R \cdot Q$$ - Arteries: carries blood away from the heart; the main artery is the aorta. Smaller arteries called arterioles diverge into (continuous) capillary beds, which contain 10-100 capillaries.
- Capillaries: branch among the cells and tissues of the body, and carry blood through the body and exchange nutrients, waste, and oxygen with tissues at the cellular level.
- Veins: blood vessels that bring blood back to the heart and drain blood from organs and limbs. Smaller veins called venule diverge into (fenestrated) capillary beds.
Heart valves

Ensure unidirectional blood flow. Atrioventricular valves between atrium and ventricle (mitral / bicuspid valve - left side; and tricuspid valve - right side) are open during filling and closed during ejection. Arterio-ventricular valves between ventricles and arteries (aortic valve - left side; and pulmonary valve - right side) are open during ejection and closed during filling.
Circulatory system diseases
Valvular disease:
- Insufficiency / reguritation (leakage)
- Stenosis (narrowing). Valve diseases in the left side has more consequences due to higher pressures and pressure differences.
Arterio-ventricular valve disfunction:
- Leakages in diastole → increase filling volume into ventricle → ventricular volume overload
- Stenosis in systole → increase resistance against ejection → ventricular pressure overload
Atrioventricular valve disfunction:
- Leakages in systole --> increase atrial pressure and volume and increase filling volume into ventricle --> atrial overload and ventricular volume overload
- Stenosis in diastole --> increase atrial pressure --> atrial pressure overload

High blood pressure (hypertension): risk factor for development of vascular disease, heart infarction, heart failure, stroke. Treated by mediscines that reduce contraction force and heart rate (beta blockers blocks receptors in heart for sympathetic transmitters) and peripheral resistance.
Atherosclerosis [no: åreforkalkning]: risk factor for development of stroke in the brain, angina pectoris (chest pain, insufficient blood flow to the heart muscle during activity) and infarction in the heart, and renal failure in the kidneys.
Scientific methods in medicine
- Medicine = body function and structure + mechanisms of disease + diagnosis of disease + treatment
- Medical practice vs. medical science
- Evidence based medicine (EBM) = individual clinical judgement + external scientific evidence + patient expectations, values and context.
Epidemiology

- Epidemiology = patterns (occurence and spread), cause and effects of health and disease. Only relations, not causality.
- Confounding factor is an extraneous variable in a statistical model that correlates (directly or inversely) with both the dependent variable and the independent variable. E.g. wine give better health, rather social status.
Purpose of epidemiological research:
- Descriptive epidemiology: describe the occurrence of disease.
- Analytic epidemiology: idetify the causes of disease.
Study measures:
- Prevalence: (How many are ill?) The proportion of the population having a disease at a specific time.
- Incidence: (How many fall ill?) The number of new cases of a disease during a specified time period.
- Risk: incidence proportion. E.g. the 1-year risk of hip fracture among elderly women is 5%.
- Incidence rate: the ratio between incidences and the sum of individual follow up times. E.g. We follow a population of 10 000. During a follow up time of 10 years, 40 individuals get lung cancer. The sum of the follow up times is 100 000 person-years. Incidence of lung cancer = 40/100 000 person-years.
Types of observational studies:
- Cohort study: comparison of disease frequency between groups with different exposure.
- Case-control study: comparison of exposure between people who have fallen ill (cases) and a comparison group without the disease (control).
Clinical studies
- Treatment evidence. E.g. in treating blood pressure or high cholesterol you want to treat the risk of stroke and heart disease. The first is surrogate end point and acts as measures of treatment, while the last are the real end point.
- Placebo effect = expecting to be better, makes you better.
- Nocebo effect = expecting to be worse, makes you worse. Should be: prospective (not retrospect, goes forward in time), controlled (with control group), randomised (similar groups) and double blind studies (both patient and investigator are blinded).
- Statistical significance: the probability of finding this result given that the effects are random. Usually p < 5%.
- Study power / strength: the ability for a given study to detect an effect with a given significance. Usually 80-90%.
- Type 1 error: a random result is taken as real.
- Type 2 error: not discovering an effect that is real.
Diagnostic tests
- Methods: history, clinical examination, chemcial measurements, measurements of electrical potentials, imagin and tests.
- Validity (accuracy, high validity means unbiased mean) and reliability (precision, high reliability means small variance). Intraobserver = done by same observer. Interobserver = done by different observers.
- Kappa coefficient: a measure of agreement
$$\kappa = \frac{\text{observed agreement}-\text{expected agreement}}{1.0 - \text{expected agreement}}.$$ - Sensitivity: Probability of having a positive test if you are ill.
$$\text{sensitivity} = \frac{\text{true positive}}{\text{all ill}}.$$ - Specificity: Probability of having a negative test if you are healthy.
$$\text{specificity} = \frac{\text{true negative}}{\text{all healthy}}.$$ - Positive predictive value: Probability of being ill if you have a negative test.
$$\text{positive predicitve value} = \frac{\text{true positive}}{\text{all positive}}.$$ - Negative predictive value: Probability of being healthy if you have a negative test.
$$\text{negative predicitve value} = \frac{\text{true negative}}{\text{all negative}}.$$
Advanced Treatment in Cardiology [EMPTY]
The Digestive System

Normal structure and function
Degrade the molecules into small building blicks that can be absorbed. Tube from mouth to anus + liver + pancreas. The tube consist of (from inside to outside): mucosa, nerve plexa (regulate secretion and absorption), inner muscle layer, outer muscle layer, mesentery (attach to body nerves and blood vessels).
The tube
It has area 600 times the area of a smooth cylinder due to folds (x3), villi (x10) and microvilli (x20).
- Esophagus: transport.
- Stomach: add acid, prepare.
- Duodenum: meets bio, digestive enzymes from pancreas and the gastrointestinal tube itself. Digestive process start.
- Small intestine: digestion and absorption.
- Large intestine: mainly absorbs fluid and electrolytes ()
- Rectum
Blood flow
Blood lows in through arteries and out through the liver for cleaning and then to the systemic system.
Basic functions
- Motility (feel bolus → peristaltic wave: contract mouth side and relax anal side)
- Secretion
- Digestion
- Absorption
Diagnostic methods
Basic clinical examination: talk and examine with bare hands.
Radiology: gives patient contrast and pills that give out gas to extend the stomach. If cancer: stiff and unmoveable.
Endoscopy: Tool consist of light, camera, working channel. From mouth to duodenum, or from anus and up 10-15 cm.
Tools introduced through the working channel could be:
- systems to suck out fluid / install air / wash with water
- biopsy forceps
- snare (cutting mode: continouos sinus mode current; coagulation mode: interrupted current 50-100 Hz in square pulses)
- hemoclip.
Other methods:
- Small intestinal examination with enterocapsule for areas unaccesible through mouth or anus
- Small intestinal examination with balloon enteroscope
- manometry and pH in the oesophagus.
Example of diseases (and therapies)
- Reflux oesophagitis: inflamation → scaring → smaller and smaller.
- Gastric ulcer: hole in mucosa. Major complications are bleeding, perforation and obstruction.
- Crohn's disease
Overdiagnosis
Medical diagnostics
- Symptoms
- Incidental findings: finding when looking for something else.
- Screening: looking for disease in people without symptoms. Wild sreening or systematic screening programme.
Health status vs test result
- False positive is not the same as overdiagnosis since they are disproved by second more precise test.
- Number needed to treat (NNT): E.g. 10 000 in clinical study, mortality reduction with treatment 25 %, mortality without treatment 10% (i.e. 1000) → absolute mortality reduction
2.5% (250). Must treat 10 000 to save 250 = treat 40 to save 1.
$\text{NNT} = 40$ . - Increased use of diagnostics gives a greater number of patients that shall be treated, but still the same amount which really needs treatment since many can go their whole life without reaching the lethal phase or not even the symptomatic phase. Increased NNT.
- Strategies: 1) Agressive: all diagnosed are treated; and 2) Conservative: follow up assessment without treatment, then when reaching intervention cut-off point the treatment is started.
Electrocardiography (ECG)

Electrocardiography is the process of recording the electrical activity of the heart over a period of time using electrodes placed on a patient's body. These electrodes detect the tiny electrical changes on the skin that arise from the heart muscle depolarizing during each heartbeat.
The fundamental elements:
- P: atrial activation
- PQ-interval: conduction through AV-node and atrial contraction.
- QRS: conduction to ventricles; ventricular depolarisation.
- QT-interval: plateau phase in ventricles; contraction.
- T: ventricular repolarisation.
ECG changes with disturbance in heart rythme:
-
Heart rate: > 100 is called tachycardia (not so harmful in atria since AV node limits conduction and ventricular response, but extremely dangerous in the ventricles); 50-100 is called the normal sinus rythm; and <50 is called bradycardia.
-
Extra / missed beats: harmless (have about 100 per day).
-
Atrial fibrillation: fast, irregular atrial activation. AV node limits ventricular response.
ECG changes with disturbance in impulse conduction:
-
Sinus node stop giving pacemaker signals: harmless above AV node since AV node is reserve pacemaker (at slightly lower rate). Extremely dangerous below AV node since cause very slow rate or non at all.
-
ECG changes with disturbance in heart muscle: pump failure due to mechanical reasons.
X-ray
X-rays
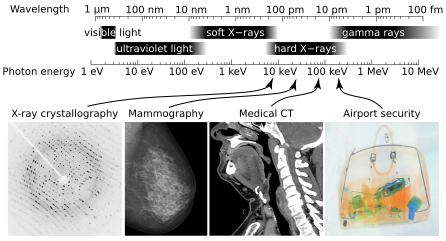
- X-rays: a form of ionising radiation that can penetrate the body to form an image on film.
- Generation: cathode rays (electrons) hit a metal anode and causes the energy of the electrons, achieved by acceleration in an electrical field, to be converted to electromagnetic radiation (energy from deceleration→continouos radiation spectrum, not quantum mechanical).
- Positive image it is black where the radiation is absorbed and white where it is transmitted, while negative image is the opposite.
- Attenuation depends on: Radiation energy (wavelength and intensity), tissue absorption.
- Diverging rays cause: enlargement of object closest to the rays source.
Computer tomography
- 1st generation:
- 2nd generation:
- 3rd generation:
- 4th generation: full ring of stationary receptors, only the tube rotates. Scan time < 1 second.
Nuclear imaging
- Basic principle: a gamma ray emitting isotope is introduced into the body. It concentrates in the desired part of the body. Radiation from that organ is detected by a gamma camera. Intensity is proportional to the amount.
- Single Photon Emission Computer Tomography (SPECT): uses mainly (99)Technetium which has a half-life of 6 hours. Technetium is also very reactive - it binds to many different chemiccal compounds that have affinity for different tissues making it very useful for imaging of most organs.
- Positron Emission Tomography (PET): positron emitting isotopes like (18)Flourine with a half-life of 110 minutes. The positrons travel a very short distance before they hit an electron and annhilates to produce two gamma photons with exactly opposite direction. These photons are detected by a ring of detectors around the patient and the concentration of the isotope is mapped by the intensity of raditation in the cross section.
MRI - Magnetic Resonance Imaging

- Structural MR: depict normal and abnormal anatomy and structure.
- Functional MR: depict normal and abnormal physiological / biological processes (diffusion, perfursion).
- MR Spectroscopy: map metabolism. -Basic principle: based on the precession of the magnetic moment in protons, more precisely in hydrogen nucleus in the water molecule. More than 60% water in the human body. Each proton has a magnetic moment due to spin and electric charge. The net magnetic moment from all individual spins are called the magnetisation. Whenever a spin moves between two energy states, energy is absorbed or released as electromagnetic radiation.
- Application of rotating magnetic field: cause the magnetisation vector to start to precess around the total magnetic field. After the radiofrequency pulse, the spin magnetisation will relax back to its equilibrium state (regrowth back to longitudinal magnetisation). This effect is called T1-relaxation. The transversal component usually disappears faster than expected, and this is called dephasing, T2-relaxation, transverssal relaxation or spin-spin relaxation.
$T_2 \leq T_1$ . [#] The gradient coils in a MR system which allows for spatial encoding of the MR signal
- Slice selection: gradient applied during radio frequency transmission. Only areas where resonance frequency fits the pulse is excited (z-axis).
- Frequency encoding: gradient applied during radio frequency reception. Protons spins at different frequencies depending on their position along the x-axis.
- Phase encoding: gradient applied between transmission and reception. After the gradient is switched off, all protons will spin with the same frequency again, but a phase shift is introduced along the y-axis.
- T1-contrast makes bone white, water black, while T2-contrast makes bone black and water white.
Ultrasound [NOT COMPLETE]
- Ultrasound is sound waves with frequency > 0.2 MHz
- Ultrasound images represent the echoes we get back when short high frequency pulses are sent into the body
- Can be used on almost any organ
- Image resolution depends on probe size and frequency
- Thermal effects: local and temporal temperature increases
- Termal index T1 = temperature increase (T1 < 3)
- Mechanical index M1 wanted < 1.9
- Doppler: When the ultrasound pulse hits a moving object, the frequency (wavelength) of the reflected signal is proportional to the velocity of the object
- Doppler shift
$\text{f}_d = 2\text{f}_0 v \cos(\theta)/c$ - Wavelength L = propagation speed c / frequency f [#]
- Doppler shift
- Frame Rate: Frame rate dependence on the number of scanlines in the imaging plane. To aquire a 3D volume instead of a 2D plane, you want to maintain the same number uf scanlines, but the frame rate wil be reduces to by a square factor
- Reducing gives a higher fram rate
- Increasing gives a lower fram rate.

Oxygen uptake [NOT COMPLETE]
- Oxygen is taken up by lungs, blood is oxygenated, transported to circulation, used by tissues, then replaced in the lungs.
- Hemoglobin: Normally about 14.8 g/dL and 1 g Hgb bind 1.4 mL
$\text{O}_2$ . The oxygen carrying capacity depend on blood volume and hemoglobin amount. - Fick's formula:
$\text{VO}_2$ = CO * ($\text{O}_2$ extraction) -
$\text{VO}_2$ =$\text{CO}$ *$\text{Hgb}$ *$1.4$ * (Arterial oxygen saturation - Venous saturation)/(body weight) -
Maxiumum oxygen uptake can be increased with endurance training, and generally requires an increased Cariac Output. As Max Heart Rate is proportional with age, this can be done mainly by increasing the max stroke volume.
Physical Training
- Physical activity: any activity except sitting and laying down.
- Training: activity at certain intensity.
- Endurance training: maximal oxygen uptake (increased by increasing stroke volume since maximal heart rate cannot be trained), anaerobic threshold, work economy (do more for the same
$\text{VO}_2$ max). - Strength / resistance training: 1 RM = the maximal weight we can lift once. 1 RFD (rate of force development) = start strength; how quickly you reach max force.
- Endurance training: maximal oxygen uptake (increased by increasing stroke volume since maximal heart rate cannot be trained), anaerobic threshold, work economy (do more for the same
- Hypertrophy: useful training vs overtraining
- Physiological hypertrophy: training - intermittent. Restitution between bouts.
- Pathological hypertrophy: constant overload. No restitution.